Announcing Version 2 of the “expedited” ISNCSCI (E-ISNCSCI)!
| In 2020, ASIA’s International Standards Committee posted the first “expedited” ISNCSCI (E-ISNCSCI) instructions on the ASIA website. The goal of the E-ISNCSCI is to determine the neurological level of injury (NLI) and ASIA impairment scale (AIS) with the fewest possible exam steps. Since then, the International Standards Committee has completed additional research about the accuracy of the E-ISNCSCI and communicated with the SCI professional community regarding testing instructions and recommended use. As a result, a new and improved E-ISNCSCI (version 2) has been released which is replacing the original E-ISNCSCI (version 1).
The E-ISNCSCI version 2 includes a full test of key muscle functions and introduces a different sequence of sensory testing. It requires additional steps compared to version 1, but still far less than a full ISNCSCI exam. Some of the changes were made to avoid unacceptably high rates of classification errors that occurred with version 1. There is no longer the option of a S1 sensorimotor exam substitution for the anorectal exam, nonetheless in the new version, not all parts of the anorectal exam are always necessary. Inclusion of full motor testing has been deemed more clinically useful by practitioners in the field, and allows for the calculation of sum motor scores. We hope the SCI professional community will appreciate this new and improved E-ISNCSCI version 2.0 and use it appropriately. Here’s to the new exam’s combination of speed, accuracy, and clinical utility! |
Expedited International Standards for Neurological Classification of Spinal Cord Injury, Version 2 (E-ISNCSCI-V2)
International Standards Committee of the American Spinal Injury Association, June 2025
Rationale
While the full ISNCSCI exam will remain the gold standard for evaluation and documentation of spinal cord injury (SCI), there are circumstances when a shorter exam may be used. The goal of the expedited ISNCSCI exam (E-ISNCSCI) is to accurately determine the neurological level of injury (NLI) and the American Spinal Injury Association (ASIA) Impairment Scale (AIS) with fewer exam items, when applicable. Although E-ISNCSCI Version 1 determined the NLI and AIS with a greatly reduced number of exam items, some shortcomings were identified in terms of accuracy, e.g., inaccuracy of AIS determination when S1 findings are substituted for the anorectal exam. Version 2 represents an improvement that better balances shortening the exam, maximizing accuracy, ensuring teachability, and satisfying clinicians’ desire for clinical information beyond NLI and AIS, namely a fuller description of motor function.
Application
The E-ISNCSCI is NOT intended to replace the full ISNCSCI exam, which should be used for comprehensive characterization of SCI in both clinical and research settings. Also, the E-ISNCSCI is not designed to produce an accurate classification in the presence of non-SCI conditions affecting exam findings or if any exam items are non-testable. The E-ISNCSCI exam is not sufficient if full ISNCSCI data collection is required or if classifications other than NLI and AIS are needed, e.g. zone of partial preservation (ZPP). Use of the E-ISNCSCI exam requires knowledge of and training in the full ISNCSCI exam, and use of the E-ISNCSCI exam by inexperienced evaluators is NOT recommended.
| Full ISNCSCI | E-ISNCSCI-V2 |
|
|
TESTING PROTOCOL
All motor testing is performed with the patient in a supine position. Typically, the patient is placed in a side-lying position for S4-5 testing, as well as for the digital anorectal exam, if required. The exam steps performed are recorded on the full ISNCSCI exam worksheet, with notation in the comment box that the neurologic classifications are based on the E-ISNCSCI-V2.
Neurological Level of Injury (NLI)
Motor testing:
- Perform motor testing for the 10 key muscles bilaterally, as per standardized ISNCSCI instructions
- Consider also testing non-key muscles at this step if it is suspected the exam may be classified as AIS B.
- Identify the presumed motor level on each side, based on motor testing only. If presumed motor levels are asymmetric, identify which one is more rostral.
- “Presumed motor level” is defined as the most caudal muscle that is at least 3/5 with all more rostral muscles testing as normal (5/5), with the following two exceptions: If motor is less than 3/5 at C5, then the presumed motor level is C4; if upper extremity muscles are all normal (5/5) and L2 is less than 3/5, then the presumed motor level is L1. The presumed motor level based on motor testing alone may not be the true motor level, since motor level can be dependent on sensory level.
Sensory testing:
- Begin with light touch testing at C2 on the side with the more rostral presumed motor level. If presumed motor levels are symmetric then begin testing at C2 on either side.
- Proceed caudally with light touch testing until either:
- A dermatome score of 1 or 0 is found, or
- The segment corresponding to the presumed motor level is reached and has been tested.
- Next, test pinprick on that same side at the most caudal dermatome that had a score of 2 (normal) for light touch in the prior step. Continue testing rostrally for pinprick until 2 consecutive dermatomes with normal pinprick sensation are identified.
- Next, test light touch on the contralateral side, beginning at the dermatome corresponding to the most caudal dermatome of the two consecutive dermatomes on the first side that tested as normal for both light touch and pinprick. Continue testing rostrally until 2 consecutive dermatomes with normal light touch sensation are identified.
- Finally, test pinprick on this second side, beginning at the dermatome corresponding to the most caudal dermatome that was tested as normal for light touch over two consecutive dermatomes in the prior step. Continue testing rostrally until 2 consecutive dermatomes with normal pinprick sensation are identified.
NLI determination:
Review the results of the motor and sensory testing in the prior steps. Assume that all untested dermatomes rostral to the tested ones are normal. Use conventional ISNCSCI criteria for NLI determination. The NLI is the most caudal segment with intact sensation and antigravity muscle function strength, provided that there is normal sensory and motor function rostrally.
ASIA Impairment Scale (AIS)
The principles for determining the AIS are nearly identical to the method described for the full ISNCSCI, other than allowing omission of some components when findings will not affect the AIS classification
Anorectal Exam Testing:
- S4-5 sensory testing:
- Perform sensory testing for light touch and pinprick at S4-5 bilaterally.
- If any light touch or pinprick sensation is found to be present at S4-5, then the remainder of S4-5 sensory testing can be omitted.
- Digital rectal exam for deep anal pressure (DAP) and voluntary anal contraction (VAC)
- If sensation is completely absent at S4-5 then check DAP and VAC
- If any sensation is present at S4-5 but motor is not preserved more than 3 levels below the motor level on either side, then check VAC
- If any sensation is present at S4-5 and motor is preserved more than 3 levels below the motor level, then DAP and VAC can be omitted
AIS Determination:
- If sensation is completely absent at S4-5 bilaterally, DAP is absent, and VAC is absent, then severity is AIS A
- If any S4-5 sensation or DAP sensation is present, but there is no motor preserved more than 3 levels below the motor level on either side, then severity is AIS B
- This includes VAC and both key and non-key muscles more than 3 levels below motor levels. If non-key muscles were not assessed when motor testing was performed, then they need to be checked at this step
- If prior criteria for AIS A and B are not met, then injury severity is motor-incomplete (AIS C or D). Count the number of key muscles below the NLI that have strength of 3/5 or greater
- If less than half of the muscles are 3/5 or greater, then severity is AIS C
If at least half of the muscles are 3/5 or greater, then severity is AIS D
Infrequent requirement for additional sensory testing:
- This testing protocol is designed to identify NLI and AIS. It will omit sensory testing that is not needed for determining the NLI. If sensory level classifications are required to allow for AIS determination, then additional sensory testing can be performed.
If there is any doubt as to the accuracy or reliability of the E-ISNCSCI exam, a full ISNCSCI exam should be performed by a trained evaluator.
References
Burns SP, Walden K, Kirshblum S, Schmidt-Read M, Tansey K, Schuld C, Rupp R. Development and Validation of an Algorithm for Item Reduction of the International Standards for Neurological Classification of Spinal Cord Injury Examination to Determine Level and Severity of SCI. Top Spinal Cord Inj Rehabil. 2025 Summer;31(3):61-67. doi: 10.46292/sci25-00008. Epub 2025 Aug 22. PMID: 40873964; PMCID: PMC12376155.
>>>>>E-ISNCSCI VERSION 2 PROTOCOL FOR PRINT – CLICK HERE<<<<<
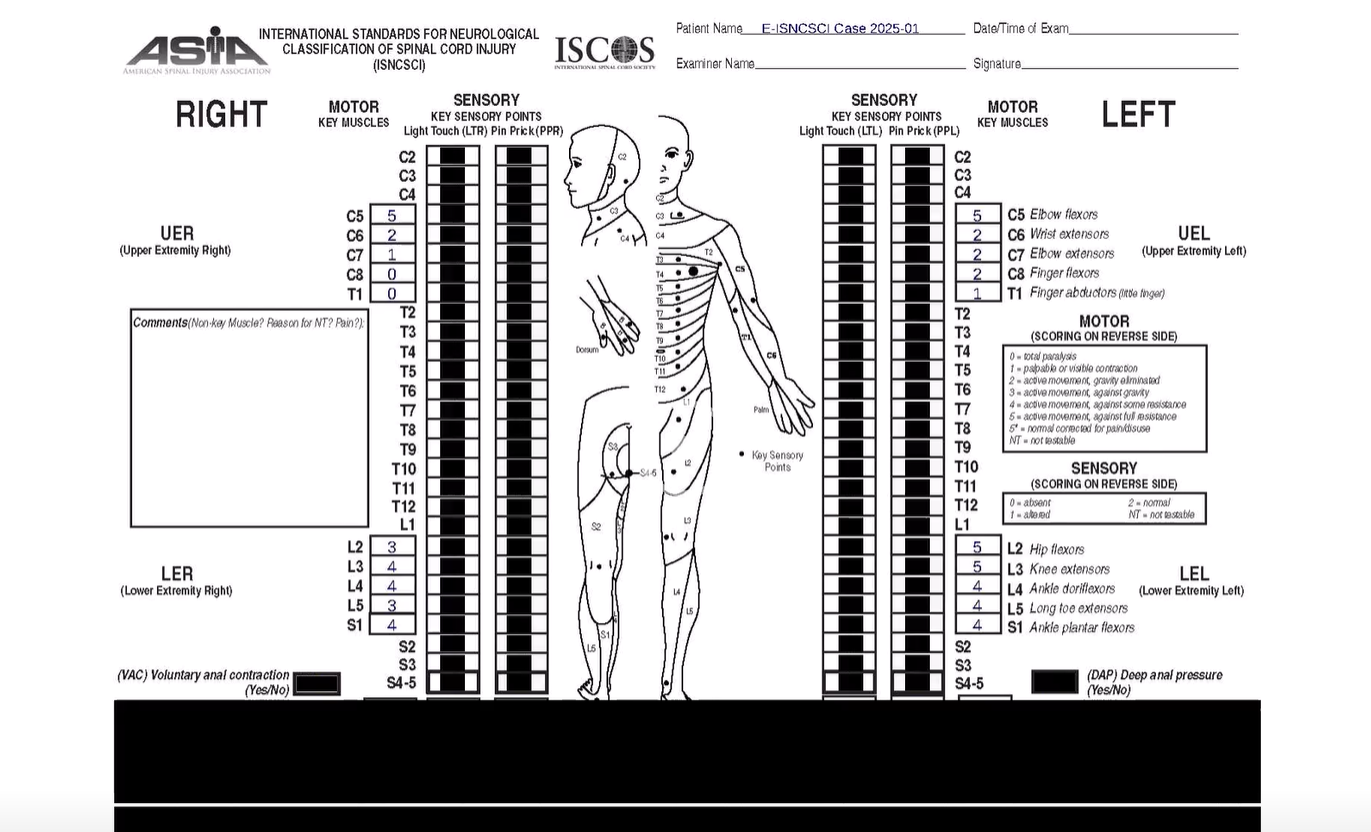
E-ISNCSCI Version 2 Cases
| E-ISNCSCI Version 2 – Case 1 |
|---|
 |
| E-ISNCSCI Version 2 – Case 2 |
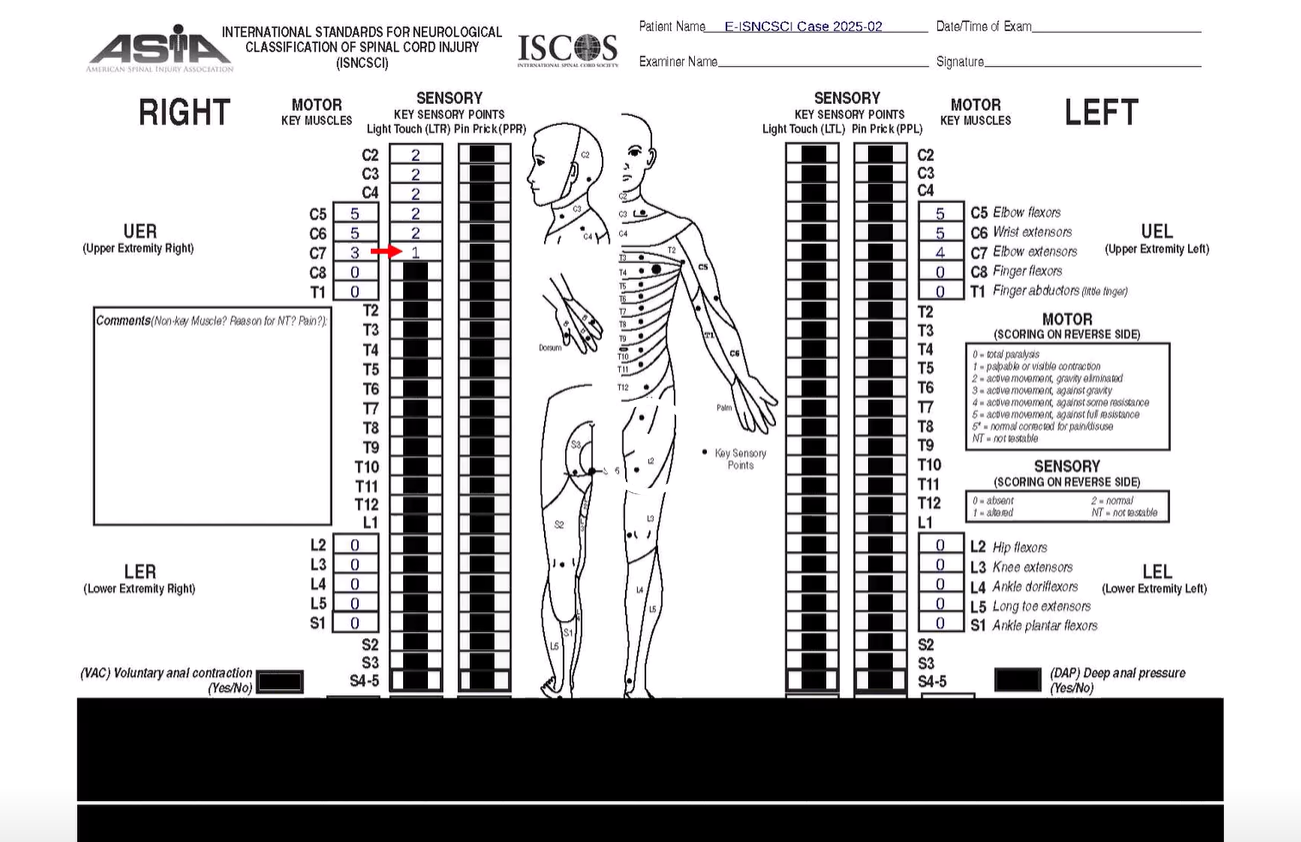 |
| E-ISNCSCI Version 2 – Case 3 |
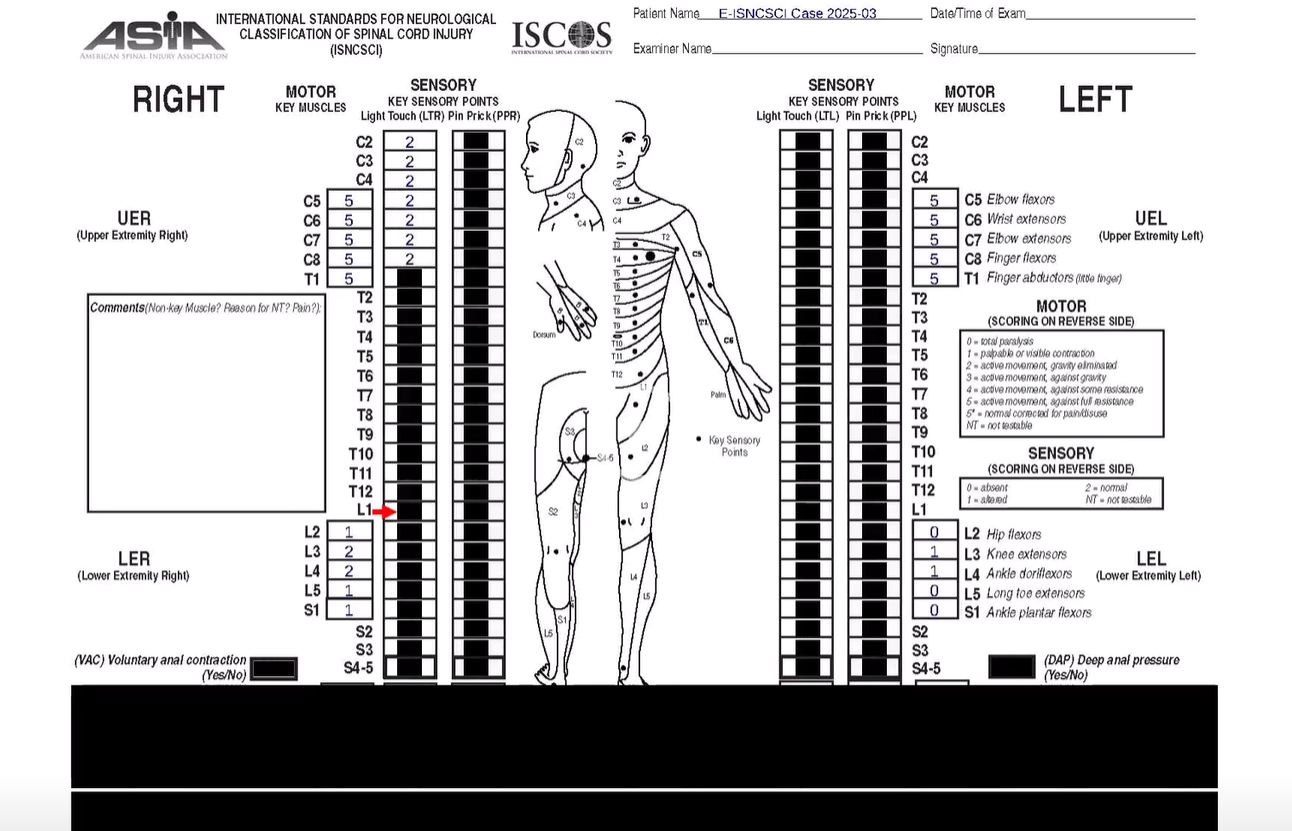 |
| E-ISNCSCI Version 2 – Case 4 |
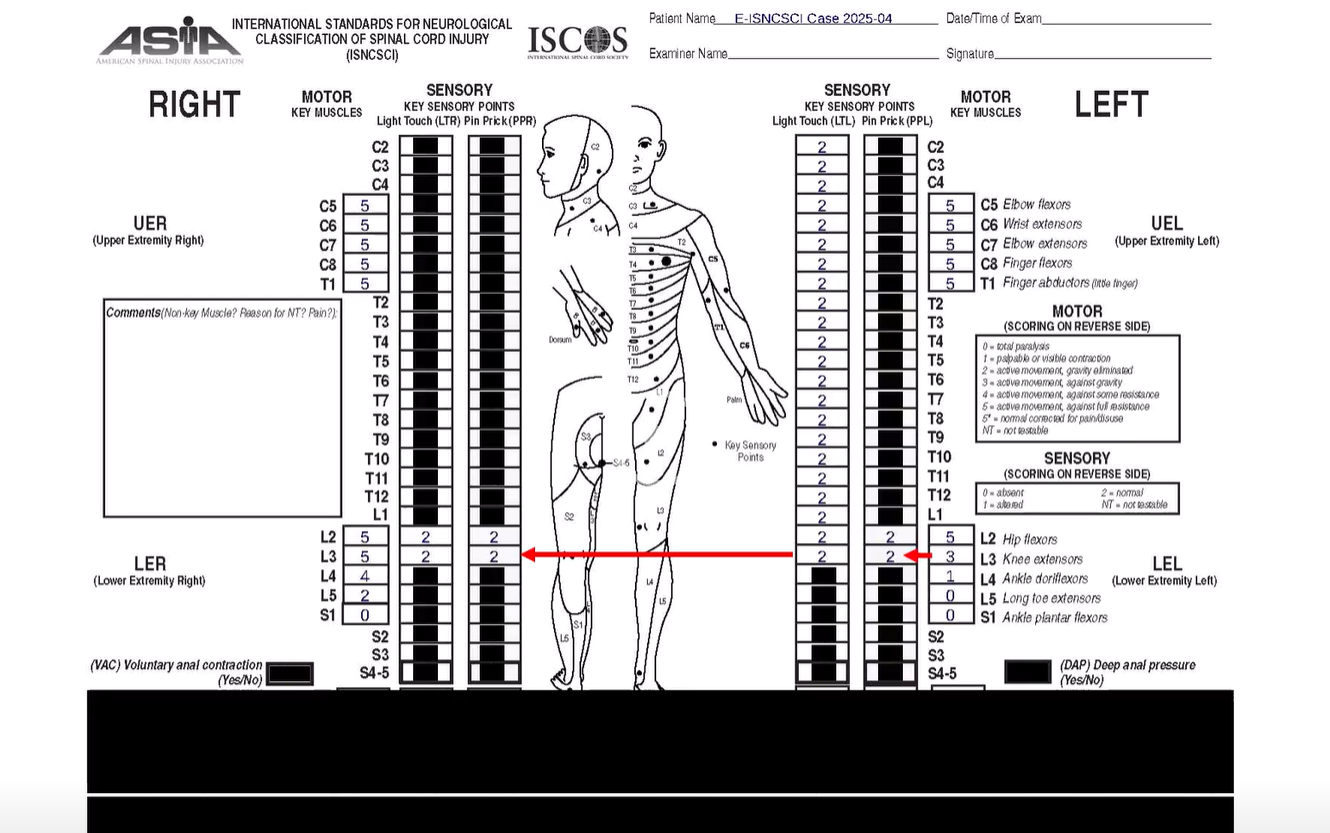 |
Contact the ASIA office – asia.office@asia-spinalinjury.org if you have any E-ISNCSCI questions or to submit a permission to reprint request.
Click here to read more about E-ISNCSCI Version 1